How to Run Your MDS Census Report
How to Run Your MDS Census Report

With the quarterly Payroll Based Journal (PBJ) submission always on the horizon, facilities have a critical checklist to complete. While submitting staffing hours is the main goal, there's an essential validation step you can't overlook: reviewing your Minimum Data Set (MDS) census.
What is the MDS Census Report?
The "MDS census review" is the internal process of verifying the list of residents CMS believes are currently in your facility. It is not a report you simply run; it's a cross-check of your records against the officialCMS count, which is derived directly from your facility's submitted MDS assessments (or lack thereof).
The most critical thing to understand is how CMS calculates this number, as their method is what creates the risk. According to the CMS PBJ FAQ(Q23), their method is to:
- Extract all MDS assessment data for your facility going back one year.
- Identify discharged residents based on submitted discharge assessments OR an interval of 150 days or more with no new assessment.
- Assume any resident who does not meet these discharge criteria still resides in the facility
That 150-day rule is the key. A resident discharged 100 days ago without a proper assessment is still counted as active. As CMS notes, this means a"Failure to submit discharge assessments will likely result in an over-estimate of actual resident census... An over-estimate of resident census will result in the calculation of lower facility staffing levels..."
The primary objective of your review is to find and correct these"phantom resident" records before you submit your PBJ data.This ensures your census is accurate, your staffing ratios are calculated correctly, and your data stands up to auditor scrutiny.
The Link Between MDS Census and a Failed PBJ Audit
This verification process is crucial for compliance and accurate reporting. PBJ auditors are paying extremely close attention to mismatches between your facility's daily census (typically from your EHR) and the officialMDS census held by CMS. Why? An MDS census count that's higher than your actual resident count is a major red flag that something is wrong with your data.
This discrepancy often points to a correctable, but dangerous error:residents have been discharged, but the corresponding MDS discharge assessments were not completed or submitted in a timely manner.
This is where the audit risk begins. When your MDS census is artificially inflated (due to these "phantom residents" who are no longer in your facility), your PBJ-reported staffing hours are divided by a larger-than-actual number of residents. This results in an inaccurate calculation of your nursing hours per resident day (HRD), which is a serious data integrity problem.
This "significant variance" is exactly what auditors are trained to look for. CMS explicitly states in its FAQ (Q26) that a failed audit can be triggered if:
...a facility did not complete all MDS discharge assessments timely, resulting in an inaccurate census calculation.
A finding like this isn't just a simple correction. This can result in a failed PBJ audit and could lead to further investigation by CMS for potential noncompliance or billing inaccuracies. In order to ensure your MDS census is correct it's important to be completing discharge assessments on every resident not included in your census.
Step-by-Step Guide to Running the MDS Census Report
PBJ reports are submitted quarterly, and facilities are expected to run their census report before submitting their PBJ information.
1. To begin, visit the iQIES website.
2. Once you have entered your login information, click on the Reports menu, and click "Find a Report".
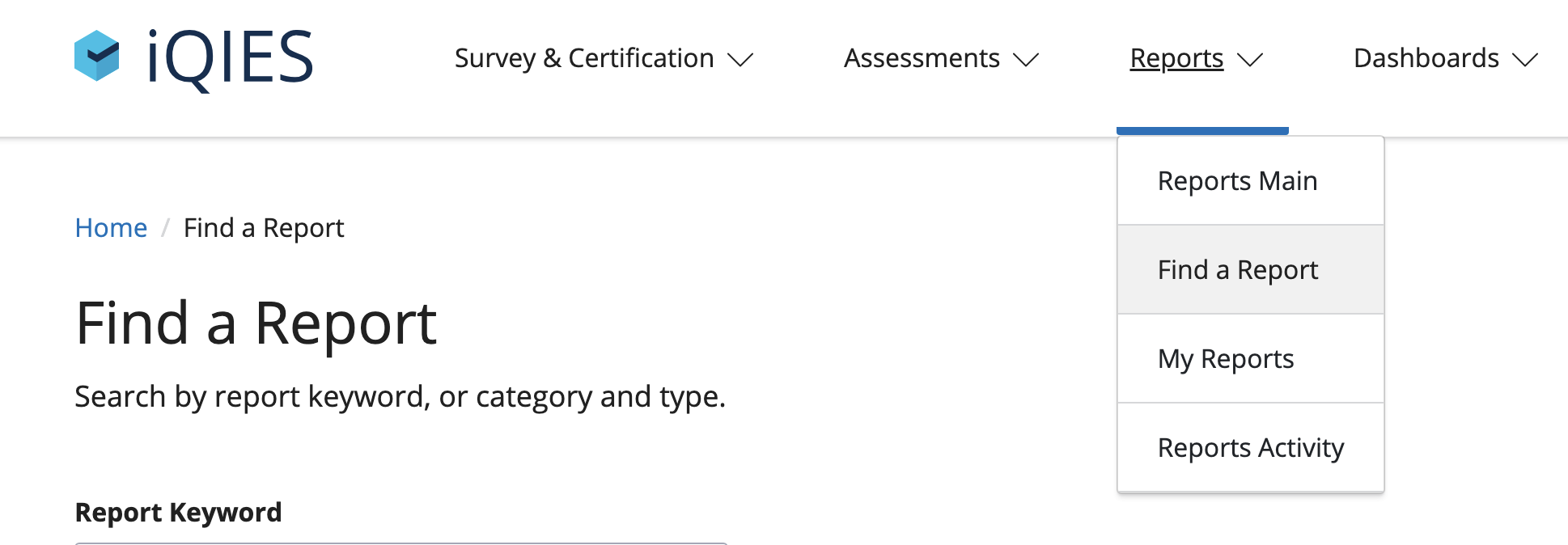
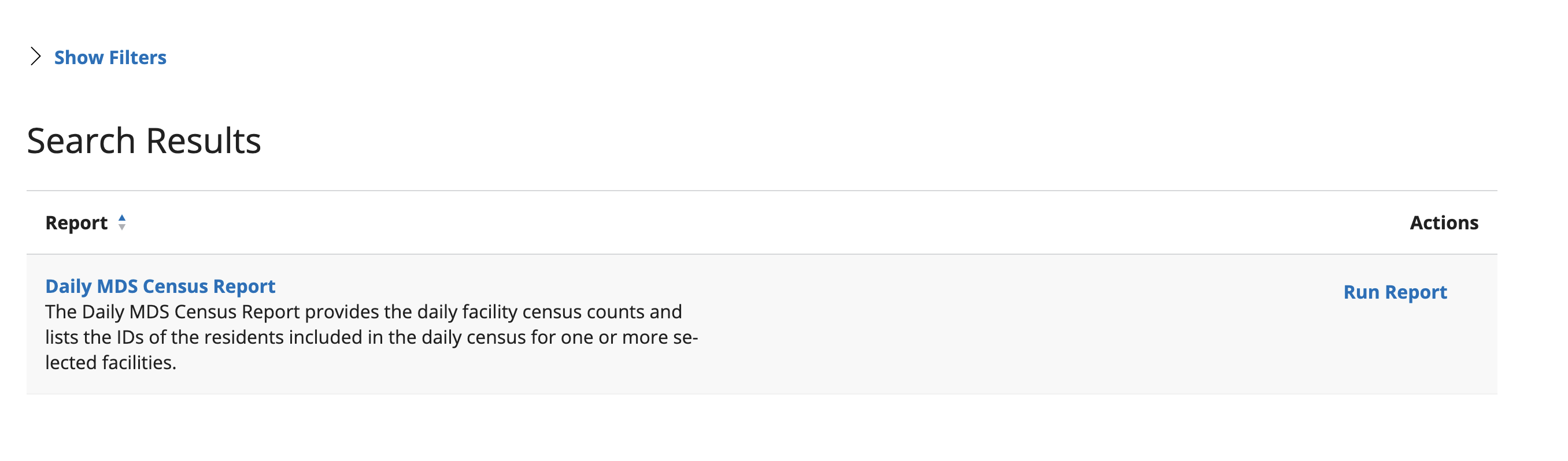
3. Under Report Type, choose “Census.”

4. The search results will bring up “Daily MDS Census Report.” Under Actions, click “Run Report.”
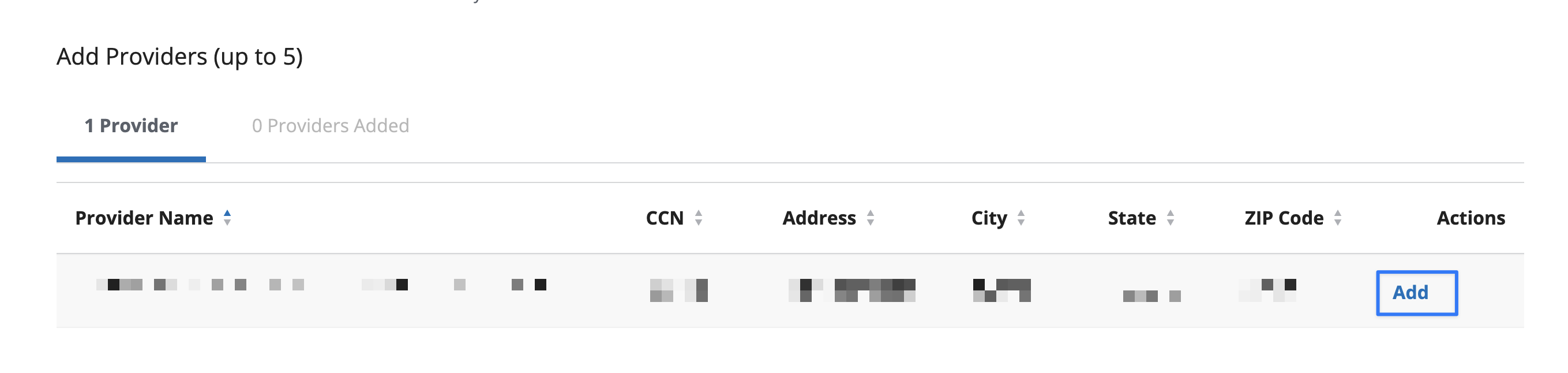
5. Select your state, and enter your facility ID.
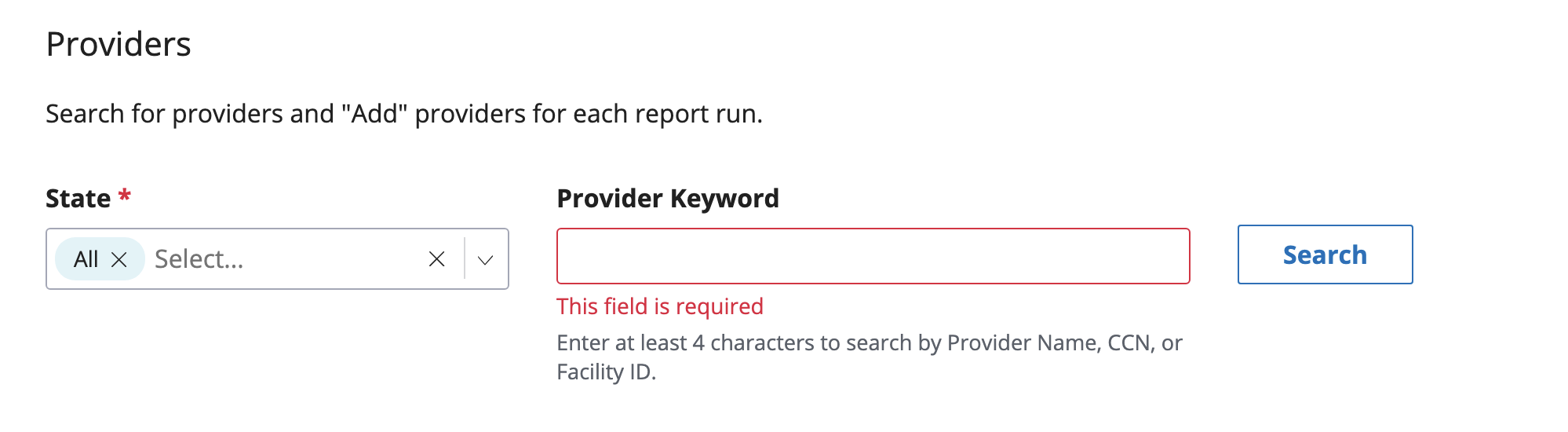
6. Once your facility appears on the screen, click “Add” under “Actions.”
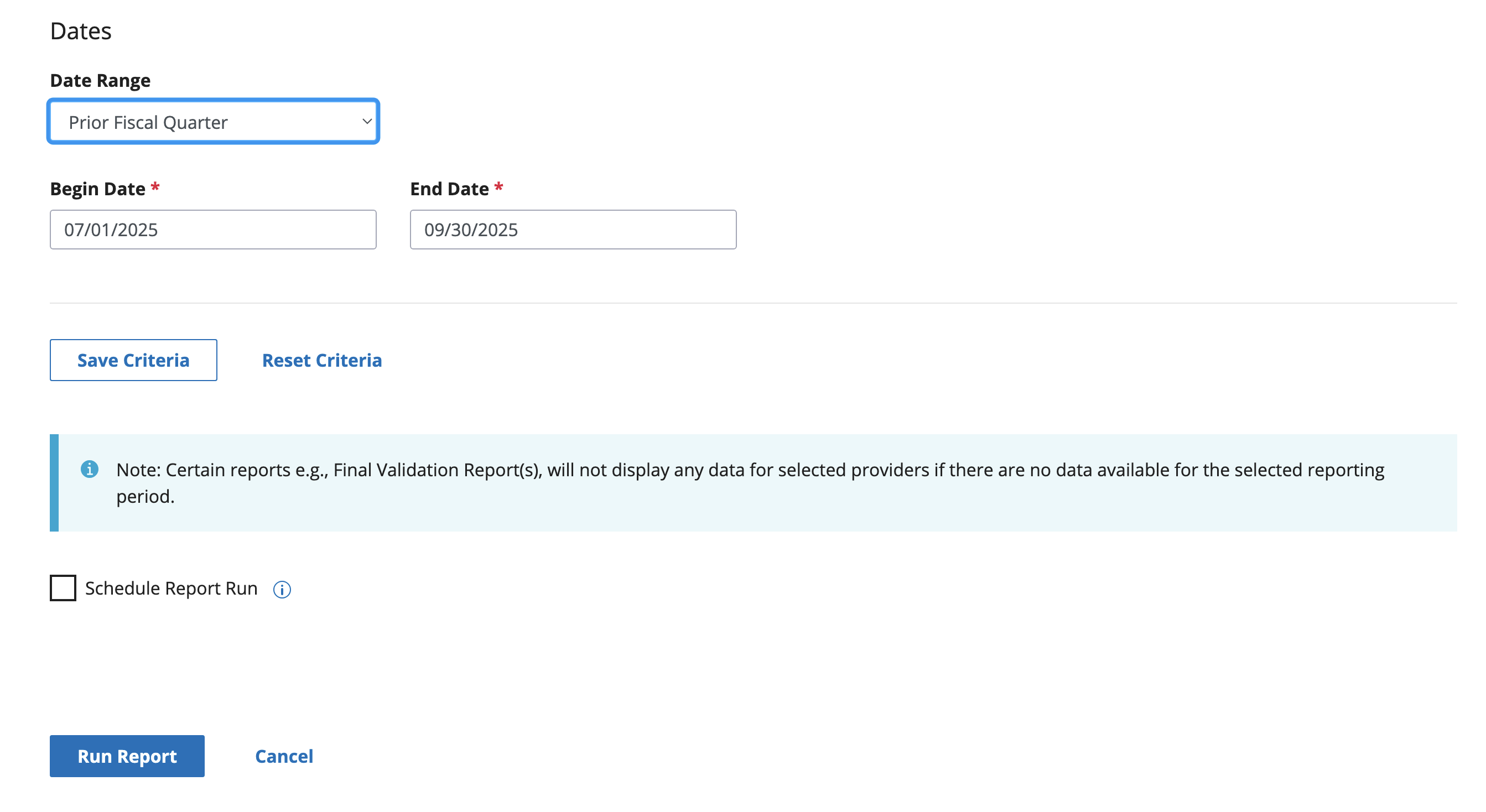
7. When choosing which dates to include, use the prior fiscal quarter.
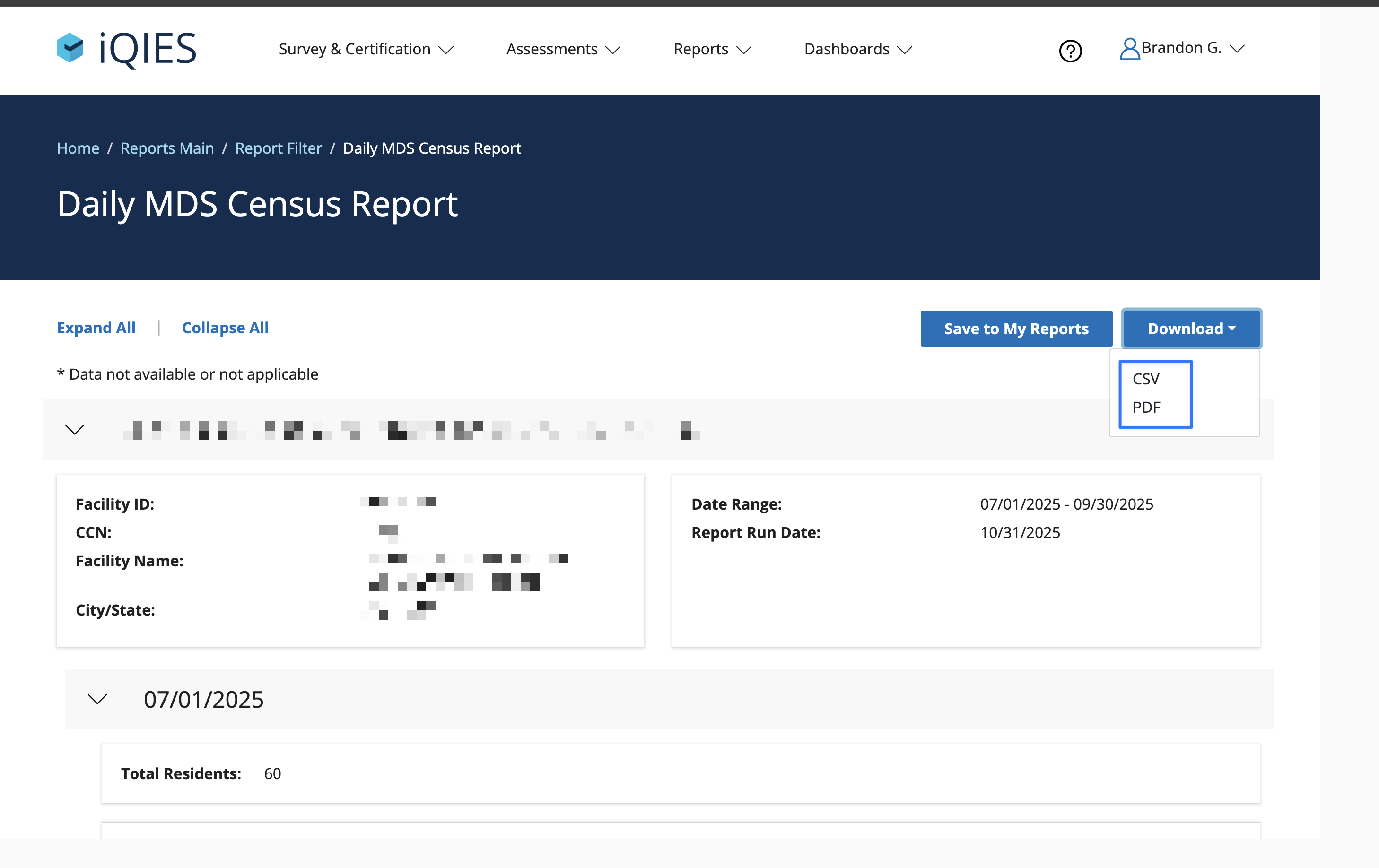
8. This will generate your report. At the top right corner, click “Download”, and you will see two options: to save your report as a PDF or CSV file. Save both files for your records.
When comparing your internal census count (per day) compared to what CMS has recorded, we've found the CSV to be a much better starting place...
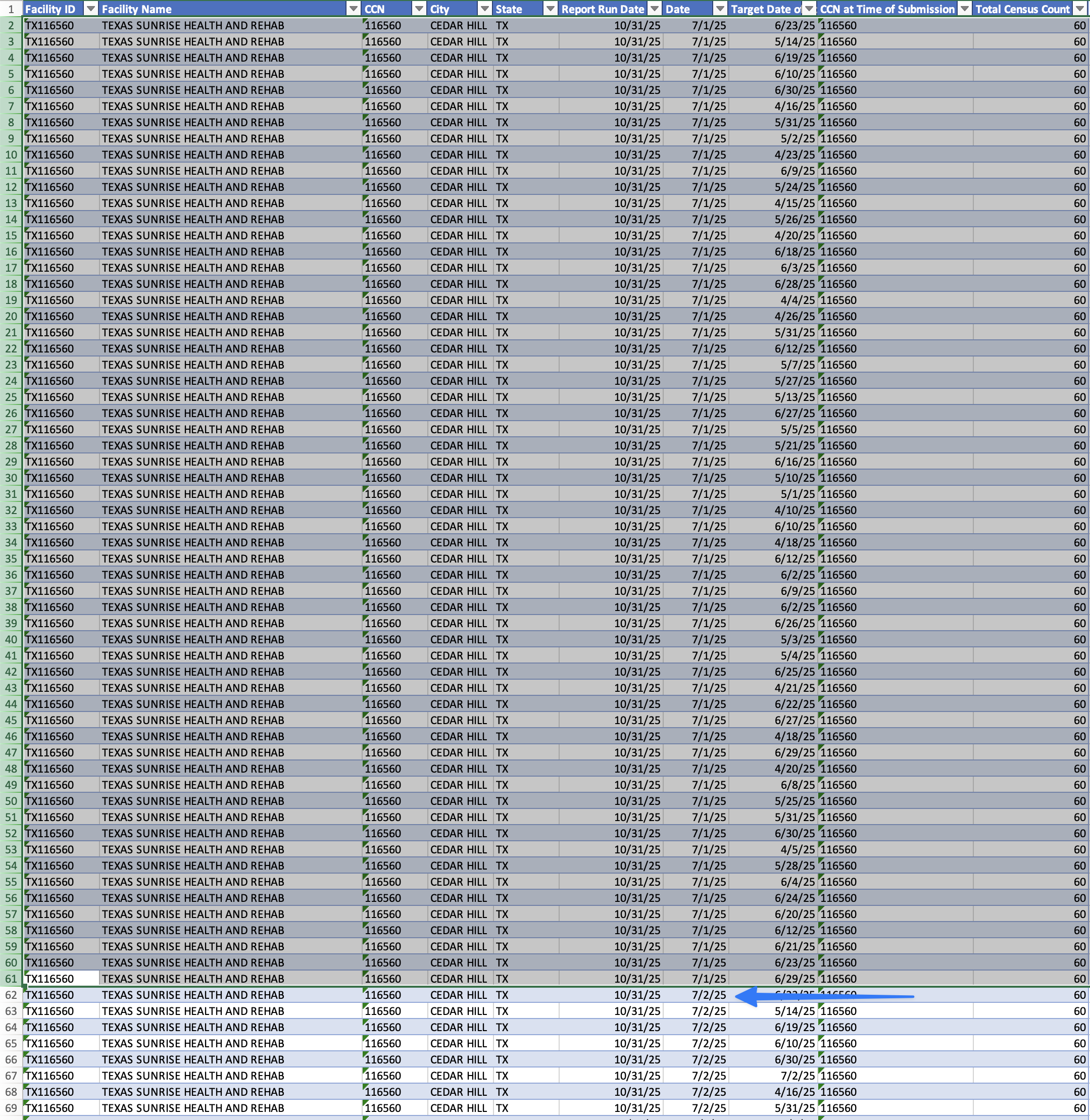
The challenge is to review this list for every day in the quarter. Once the list gets to the next calendar day, you'll need to start the audit over for that day.
Report Challenges and Troubleshooting
Unfortunately, running this report each quarter can be confusing and time-consuming. If you notice any discrepancies between your CMS census report and your facility’s daily census log, you are responsible for determining the issue and remedying it. Start by reviewing discharge assessments to find out if any are missing.
Aim to plan time each quarter to run and review your CMS census report, so that you are prepared to submit your PBJ data on time. Though the process is cumbersome, it’s an essential step in staying compliant and being eligible for the resources your facility needs.
Vast Majority of US Nursing Homes Fall Short of Meeting Minimal Staffing Requirements, According to Recent Regulations.
Vast Majority of US Nursing Homes Fall Short of Meeting Minimal Staffing Requirements, According to Recent Regulations.
A recent analysis by USA Today has found that nearly all nursing homes in the US fail to meet the minimum staffing requirements set forth by the Centers for Medicare & Medicaid Services (CMS). The analysis, which used payroll-based journal data from last August, showed that only 160 out of 14,500 skilled nursing facilities met the new requirements during the summer quarter of 2023. Furthermore, most nursing homes met the requirements on only three days out of a total of 92.
The CMS rule requires nursing homes to have a minimum of 3.48 hours per resident per day (HPRD) of total staffing, with specific allocations for registered nurses (RN) and nurse aides. However, according to the analysis, about 50% of federally funded facilities were able to provide at least 0.55 hours of care from an RN daily, while facilities were only able to provide each resident with 2.45 hours of care from a CNA on one day per week.
The gap in meeting staffing requirements was found to be significantly wider in many Southern states, with Louisiana, Oklahoma, and Texas performing the worst. In contrast, states such as Alaska, Hawaii, Utah, Maine, and Delaware fared better in meeting the total minimum staffing standard. The article notes that rural counties have five years to implement the minimum staffing standards, while urban areas are allowed up to three years.
The findings of this analysis highlight a significant challenge facing nursing homes across the US, particularly those in Southern states. The CMS rule is intended to ensure that residents receive adequate care and attention from qualified staff, but it appears that many facilities have a long way to go in terms of meeting these requirements.
Examining the Implications of the Revised Nursing Facility Rule and Identifying Facilities That May Comply with Enhanced Staffing Standards.
Examining the Implications of the Revised Nursing Facility Rule and Identifying Facilities That May Comply with Enhanced Staffing Standards.
This text appears to be a report from the Kaiser Family Foundation (KFF) analyzing the impact of new federal requirements for nursing facility staffing. Here are the main points:
Background: The Centers for Medicare and Medicaid Services (CMS) has finalized a rule requiring nursing facilities to have a minimum number of staff on duty at all times.
Key findings:
- In 45 states, fewer than half of nursing facilities have enough staff to meet the new requirements.
- About 1 in 5 nursing facilities would meet fully-implemented minimum staffing standards in the final rule with current staffing levels.
- Rural facilities are more likely to not meet the requirements compared to urban facilities.
Methodology: The analysis uses data from Nursing Home Compare, a publicly available dataset that provides information on quality of care and key characteristics for approximately 14,900 Medicare and/or Medicaid-certified nursing facilities. The analysis drops about 3% of nursing facilities due to missing data.
Limitations: The analysis does not look at facilities that meet the requirement to have an RN on staff 24 hours a day, seven days a week (24/7) due to limitations in publicly available data.
Implications: The report highlights concerns about the potential unintended consequences of the new requirements, including increased costs for nursing facilities and the potential impact on state budgets and federal spending. The need for nursing facility care is expected to increase as the population ages, which may intensify these challenges.
Overall, the report suggests that many nursing facilities face significant challenges in meeting the new staffing requirements, particularly rural facilities.
Get ready for a major update: CMS proposes a significant 4.1% pay increase for nursing homes!
Get ready for a major update: CMS proposes a significant 4.1% pay increase for nursing homes!
The Centers for Medicare & Medicaid Services (CMS) has proposed a 4.1% pay increase for nursing homes in fiscal year 2025, but declined to issue an update on its staffing minimum proposal as part of its annual payment rule proposal. The proposed increase includes a 2.8% market basket update and a 1.7% market basket forecast error adjustment, which is considered modest by industry leaders.
American Health Care Association President and CEO Mark Parkinson expressed disappointment with the proposed increase, stating that it will not be enough to offset the costs of meeting CMS's proposed staffing minimum requirement. Parkinson urged the Administration and CMS to reconsider the staffing mandate, warning that it could lead to nursing home closures and reduced access to long-term care for seniors.
The proposed rule also includes changes to the Patient-Driven Payment Model ICD-10 Code Mappings and Value-Based Purchasing updates. Additionally, CMS has proposed an expanded Civil Monetary Penalty process that would allow for more penalties to be imposed on nursing homes for health and safety violations. The agency is seeking comments on potential future updates to the non-therapy ancillary component of PDPM.
Industry leaders are cautiously optimistic about the proposed pay increase, which they believe will help offset increased labor costs associated with staffing shortages. ADVION Executive Vice President Cynthia Morton stated that the payment update reflects the increased costs experienced by providers over the past couple of years and will greatly help with recruiting and retaining staff.
The 211-page proposed rule is set to be officially published in the Federal Register, followed by a 60-day comment period. A final rule is expected to be announced by the end of July.
CMS Proposes New Rules for Nursing Homes, Including Mandatory Staffing Levels and Improved Facility Evaluations.
CMS Proposes New Rules for Nursing Homes, Including Mandatory Staffing Levels and Improved Facility Evaluations.
The provided text appears to be a webpage from the law firm Crowell & Moring's blog, specifically their Health Law section. The content includes:
- A list of recent updates and articles on various topics related to health care law, such as the attorney-client privilege waiver, information blocking, False Claims Act cases, and more.
- A sidebar with links to different categories and archives of past posts, including topics like administrative law, advertising, antitrust, artificial intelligence, COVID-19, and more.
- Information about the Crowell & Moring health care practice, including their experience in areas such as health care antitrust, managed care, fraud and abuse, and privacy litigation.
- A disclaimer and copyright notice at the bottom of the page.
The webpage is designed to provide readers with updates and insights on current developments in health care law, while also promoting Crowell & Moring's expertise and services in this area.
Latest Insights and Updates
Stay informed with our latest articles.
British study shows evidence of waning immunity to Covid-19
Imperial College London study of 365,000 people in England shows 26% decline in COVID-19 antibodies over three months, suggesting potential waning immunity and implications for long-term protection.
A study of hundreds of thousands of people across England suggests immunity to the coronavirus is gradually wearing off - at least according to one measure.
Researchers who sent out home finger-prick tests to more than 365,000 randomly selected people in England found a more than 26% decline in Covid-19 antibodies over just three months.
"We observe a significant decline in the proportion of the population with detectable antibodies over three rounds of national surveillance, using a self-administered lateral flow test, 12, 18 and 24 weeks after the first peak of infections in England," the team wrote in a pre-print version of their report, released before peer review.
"This is consistent with evidence that immunity to seasonal coronaviruses declines over 6 to 12 months after infection and emerging data on SARS-CoV-2 that also detected a decrease over time in antibody levels in individuals followed in longitudinal studies,"
The study was published Monday by Imperial College London and Ipsos MORI, a market research company. At the beginning of the study, in June, 6% of those who took the tests had IgG antibody responses to the coronavirus, they reported. By September, just 4.4% of them did. For health care workers, the rates stayed about the same.
Antibodies are the proteins your body naturally generates to fight infection. IgG are one type - the tests were not designed to detect other types of antibodies. Other research teams have found that other types of antibodies may persist longer than IgG does.
This article was originally found on cnn.com
Reporting Results of Point of Care Testing for COVID-19: A New NHSN Pathway
NHSN introduces new pathway for nursing homes to report point-of-care SARS-CoV-2 test data, enabling electronic submission to public health agencies and compliance with CARES Act requirements.
The NHSN team will introduce and provide training for a new NHSN Long-term Care Facility COVID-19 Pathway laboratory data reporting option. The October 22nd training will be live and allow for submission of audience questions. The October 23rd training will be a rebroadcast of the recorded training followed by a live Q & A session. A recording of the original webinar will be posted for on-line viewing.
The new NHSN option will enable nursing homes to enter point of care (POC) SARS-CoV-2 laboratory test data into the NHSN application. NHSN, in turn, will report the nursing home POC laboratory test data electronically to the public health agency, state or local, that has jurisdictional authority and responsibility to receive and use the nursing home’s data. Deidentified nursing home POC laboratory also will be reported via existing public health reporting mechanisms to the US Department of Health and Human Services in accordance with the U.S. Coronavirus Aid, Relief, and Economic Security (CARES) Act requirements.
This article was originally found on zoomgov.com
25-year-old man first in U.S. to catch COVID-19 twice, researchers say
First confirmed COVID-19 reinfection case in North America: 25-year-old Nevada man tests positive twice in April and June 2020, experiencing symptoms both times despite no underlying conditions.
A 25-year-old man is believed to be the first person in the United States — and North America — to be infected with COVID-19 twice, according to researchers. The man, a resident of Washoe County in Nevada, first tested positive for the virus in April and then again in June, researchers said in The Lancet Infectious Diseases, a medical journal.
The team, led by researchers from the University of Nevada and Nevada State Public Health Laboratory, said the man showed symptoms each time he tested positive.
The patient, who had no history of significant underlying conditions, first tested positive at a community testing event on April 18, when he had symptoms such as sore throat, cough, headache, nausea and diarrhea that began on March 25. He went into isolation and his symptoms were "resolved" by April 27. He then had two negative tests in May, the study said.
This article was originally found on cbsnews.com
Study Confirms It's Possible to Catch COVID Twice
Hong Kong researchers confirm first documented case of COVID-19 reinfection in 33-year-old man, with different viral strains detected in March and August 2020, demonstrating possibility of multiple infections.
Researchers in Hong Kong say they’ve confirmed that a person can be infected with COVID-19 twice.
There have been sporadic accounts on social media sites of people who say they’ve gotten COVID twice. But scientists have been skeptical about that possibility, saying there’s no evidence it happens.
The new proof comes from a 33-year-old man in Hong Kong who first caught COVID-19 in March. He was tested for the coronavirus after he developed a cough, sore throat, fever, and a headache for 3 days. He stayed in the hospital until he twice tested negative for the virus in mid-April.
On Aug. 15, the man returned to Hong Kong from a recent trip to Spain and the U.K., areas that have recently seen a resurgence of COVID-19 cases. At the airport, he was screened for COVID-19 using a test that checks saliva for the virus. He tested positive, but this time, had no symptoms. He was taken to the hospital for monitoring. His viral load -- the amount of virus he had in his body -- went down over time, suggesting that his immune system was taking care of the intrusion on its own.
This article was originally found on webmd.com
Trusted by Healthcare Leaders
Votive transforms compliance processes completely
“Our Medicare reimbursements were witheld, in error, due to non-reporting. Votive provided the proper documentation to prove we had been reporting. I was so grateful that we use such a reliable platform!”
“Streamlining our NHSN and PBJ reporting has drastically reduced the time my staff spend on compliance. It’s so nice working with one solution for all compliance requirements.”

Stay Updated with Our News
Subscribe to our newsletter for the latest updates and insights in post-acute healthcare.

Frequently Asked Questions
Find answers to common questions about us and our product
What is Votive?
How does it work?
Who can use it?
Is training included?
How to get started?